Great Disparities in Radiological Resources in African Countries
Estimates by WHO and other global health organizations estimate that about half to two-thirds of the world’s population lacks access to radiology imaging, impacting disease management, mortality, and non-invasive treatment monitoring. When you look at the data for individual African countries, you’ll see a large disparity among them. Striking first is the disparity between the US and the most advanced African country in healthcare, South Africa, which has only 27% of the radiology resources per million people compared with the US.
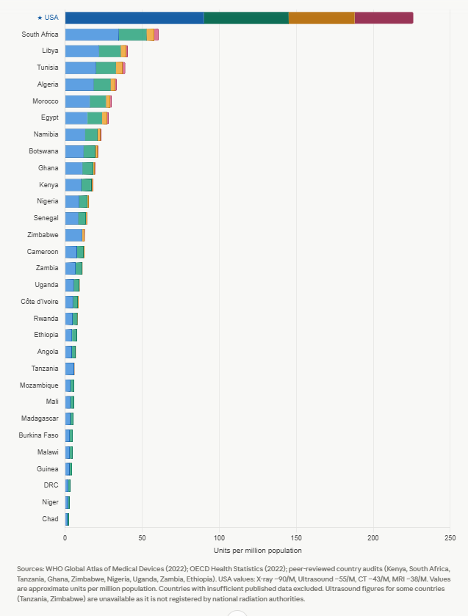
Figure 1: X-Ray (blue), Ultrasound (green), CT (orange), and MRI (red) distribution across different countries
If you look at the distribution of modalities, CT and MRI are almost absent on the African continent, especially compared with X-ray and Ultrasound. This is consistent with WHO guidelines, which specify that X-ray and US should cover about 90% of imaging needs in resource-limited settings. It is also interesting to see that the North African countries (Tunisia, Algeria, Morocco, Egypt) are comparatively well-resourced.
There are many reasons for this disparity, and as we deploy radiology in these settings, we are learning more about the challenges and the necessary conditions for successful installations. Just as an example, I have seen that the more sophisticated the equipment, the higher the chance of it being inoperable, either broken, lacking spare parts, or due to a lack of personnel resources. Basic infrastructure challenges, such as reliable power and network connectivity, are major barriers, as well as a lack of healthcare provider resources, notably physicians, specialty providers such as radiologists, and even personnel trained to operate the equipment, i.e., Radiological Technologists.
To make a difference, it is critical to assess the actual equipment situation. For example, the presence of Ultrasound has been under-reported, as the lack of ionizing radiation does not require official registration. Given limited resources in personnel and expertise, imaging AI is poised to make a significant difference in these countries by aiding disease detection and diagnosis. AI will be an inflection point for healthcare facilities, motivating them to invest in digital imaging infrastructure that supports PACS. However, none of the surveys include the presence of a PACS system, which is a requirement for AI deployment.
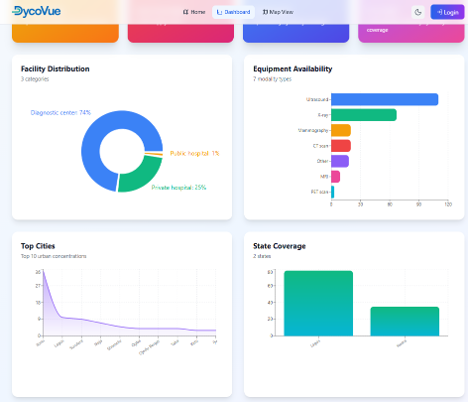
To assess the state of the art, a Geographic Information System (GIS) designed to map and evaluatehealthcare imaging infrastructure across facilities is a valuable tool. Collecting real-time data on imaging equipment, including PACS availability, workforce, and operational challenges, provides geographic visibility into gaps in diagnostic services and healthcare access.
Below are the results of a 3-month ground survey of imaging facilities across 2 states in Nigeria, conducted by DycoVue, which yielded some interesting insights. As shown in the previous chart, Nigeria ranks 11th in radiology equipment per million inhabitants. When looking at the details, including PACS availability, we’ll see that Ultrasound is the most commonly available modality, confirming the hypothesis that these units are underreported in the official statistics. The good news is that 29% of the surveyed sites have already adopted a PACS system, which bodes well for AI deployment.
There is still a lot of work to be done, especially regarding infrastructure, as the top challenge reported in this survey is power supply. As a matter of fact, I know from personal experience that most grants for deploying radiology either include a reliable power source, such as solar, or require its presence before making any investment in radiology. As many AI algorithms run in cloud environments, and support from remote experts (Teleradiology), especially when installing sophisticated devices such as a CT, is almost a necessity, access to cloud hosting companies is critical. As of today, about half of African countries prohibit the use of Starlink for Internet connections, and only a handful host data centers for cloud hosting companies such as AWS, Google, or Microsoft, which hampers cloud deployments.
Another barrier to AI deployment is that their algorithms are trained on non-local data. For example, the US FDA requires training data to be sourced from US institutions that represent a cross-section of the US's cultural, ethnic, and racial diversity. There are good reasons to believe that the performance would differ when applied to African patients, in addition to the fact that tropical diseases will likely be absent from the US-based training data set. For example, in the US, one might see 3 TB cases per 100,000 people; in many African countries, it would be several hundred per 100,000.
Despite these challenges, there is no question that imaging AI will happen in Africa; there is just too much to be gained. Pilot sites will teach us how to proceed and provide a roadmap for successful implementations.